Designing a Wellness Infrastructure for High-Demand, Incident-Driven Organizations
Date:Friday March 6, 2026
Abstract
Wellness initiatives in high-demand operational systems frequently stall despite sustained investment and genuine intent. This paper argues that these failures are not the result of cultural resistance or insufficient motivation, but of a structural mismatch between operational time horizons and the temporal nature of wellness itself. High-demand organizations operate in real time, while wellness accumulates over years through cumulative exposure and recovery. We introduce infrastructure-based wellness as a design approach capable of functioning under daily operational pressure without displacing crisis intervention. Clinicians, peer support personnel, and chaplains are positioned as long-horizon actors who carry continuity across leadership cycles and operational churn. The paper affirms crisis intervention as an essential and sustainable foundation, while outlining complementary infrastructure elements that reduce chronic strain and foster support system survivability across time and varying incidents.
Keywords wellness · psychological first aid · PFA · crisis intervention · critical incident stress management · CISM · emergency services · peer support – public safety
Most adults spend one-half of their waking lives at work. This can be a problem as well as an opportunity. High-demand, high-stress workplaces — law enforcement, fire suppression, emergency medical services, healthcare — are, by definition, high-risk environments for stress, burnout, psychological injury, trauma, and diseases of accelerated aging. Crisis intervention teams have proliferated over the past 35 years, led by the visionary work of Jeffrey Mitchell (Mitchell & Bray, 1989). Crisis response teams expanded into peer support teams, and later wellness initiatives. But the evolution and integration of these complementary services has not always been easy. This paper affirms crisis intervention as an essential and sustainable foundation, while outlining complementary wellness elements that reduce chronic strain and foster support system survivability across time and varying incidents.
Scope of the Problem: State and Trait Arousal
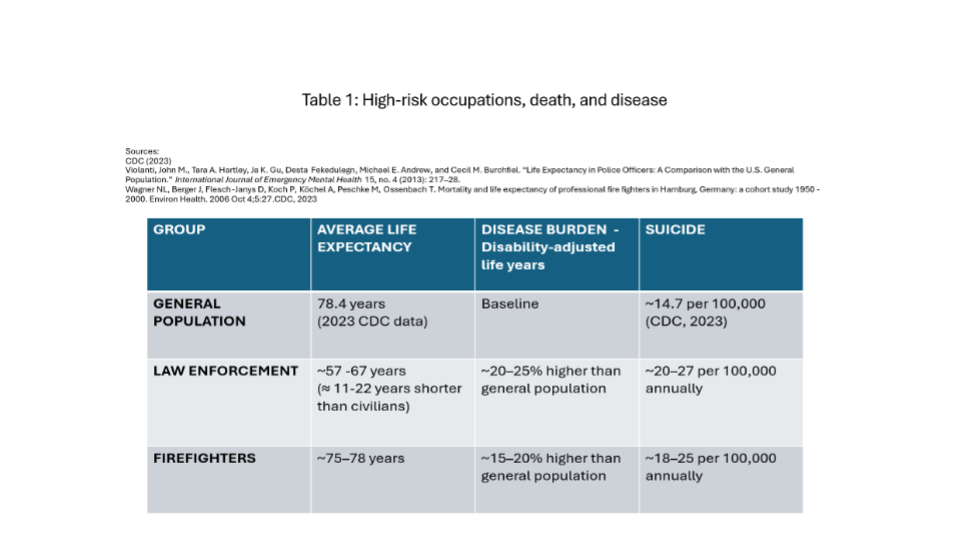
Emergency services, healthcare, and the military are professions wherein personnel must be constantly vigilant and ready to respond at a moment’s notice. This chronic trait of arousal punctuated by acute states of high-intensity activation can take a toll psychologically and physiologically. Data in Table 1 support that conclusion by revealing the association between high-risk emergency services occupations and disease and premature death.
A rationale for providing disease prevention, resilience, and wellness programs would seem self-evident. There is a powerful rationale to promote not only organizational health, but personal health, using the workplace as a platform — especially in careers that place people at high risk for physical or psychological injury such as law enforcement, fire suppression, emergency medicine, air traffic control, health care, the military, and disaster response. Careers in these and related professions might actually be prolonged, if desired.
The current healthcare system presents additional urgency. Despite having the most expensive health care system in the world, the United States ranks last overall among 11 industrialized countries on measures of health system quality, access to care, equity, and healthy lives (Commonwealth Fund, 2014). The U.S. population has a five-year lower expected life expectancy, a 50% higher disease burden on average, and 8% higher prevalence of premature death (Peterson-Kaiser Health Tracker, 2022). Major contributing factors appear to be poor accessibility and failure to provide preventative health-related initiatives.
Unfortunately, empirical analyses of wellness programs have been disappointing or mixed. A systematic review revealed low confidence that resiliency training programs have a small to moderate effect at improving resilience and other mental health outcomes (Leppin et al., 2014). A large group randomized controlled trial involving 2,831 Canadian Armed Forces recruits found no significant positive effects on resilience, psychological functioning, or military performance (Fikretoglu et al., 2019). The program appears vulnerable to highly variable quality of instruction and challenges translating classroom learning to real-world application.
Time-Scale Mismatch at the Heart of Wellness
Beyond logistical, translational, and instructional fidelity concerns, what other issues could explain these mixed findings? High-demand organizations are optimized for immediacy. Decisions are made at the pace of minutes, shifts, and calls, with leadership attention consumed by maintaining uninterrupted operational continuity. Wellness, however, unfolds on a fundamentally different timeline. Its effects are cumulative, shaped by repeated exposure, incomplete recovery, and gradual depletion of physical and psychological reserves.
This creates a structural mismatch. Organizations are designed to respond to immediate disruption, while wellness requires sustained attention across years. When wellness initiatives fail to gain traction, the cause is often attributed to culture, leadership priorities, or individual resistance. In reality, the mismatch is architectural.
Many organizational wellness models also rely implicitly on recovery occurring outside of work, assuming that individuals will self-regulate baseline capacity during off-duty hours. As off-duty recovery environments become increasingly constrained by sleep disruption, financial strain, digital saturation, and competing responsibilities, this assumption further widens the gap between operational demand and long-term capacity preservation. It takes about a week to re-establish normal circadian rhythm after working midnight shifts. Sustainable wellness models must therefore function across both on- and off-the-job conditions simultaneously.
Crisis Intervention as an Essential and Enduring Foundation
The first-response professions are often characterized by chronic stress punctuated by repeated states of crisis. Acute incidents are inevitable in high-risk professions. Individual- and organizational-level crisis intervention remains irreplaceable for stabilizing disruption, protecting personnel, and restoring functional capacity (Everly & Mitchell, 1999).
No wellness-oriented preventive or longevity-based approach eliminates the need for crisis response. Critical incident stress intervention addresses moments of destabilization that exceed baseline coping and support mechanisms. Its role is foundational.
Conversely, crisis intervention programs are designed to respond to acute disruption to psychological homeostasis, not to manage cumulative load. Critical Incident Stress Management (CISM), arguably the world’s most prevalent integrated crisis intervention system, is primarily a reactive intervention approach, albeit integrated and comprehensive in nature (Everly, 2025). Expecting crisis response to serve as a comprehensive wellness strategy places unrealistic demands on systems built for episodic activation. Crisis intervention is foundational, but it cannot carry the entire wellness burden alone.
Why Crisis-Centered Models Become Overextended
As cumulative strain increases, crisis systems are activated more frequently. This escalation is often misinterpreted as a failure of intervention models or personnel. In practice, it reflects a volume problem rather than a design flaw.
Overreliance on reactive crisis intervention signals missing upstream infrastructure. When chronic strain is unaddressed, acute disruption becomes more common. Intervention systems are then asked to absorb stressors they were never designed to carry — burnout, challenges of retirement, familial strain. This dynamic does not indicate that crisis intervention is ineffective; it indicates that it is being asked to perform a function it was never designed to carry.
Wellness as an Enduring Infrastructure, Not Intervention
Infrastructure architecture differs from intervention in several critical ways. It persists when attention drops, survives leadership transitions, and functions with minimal dependence on momentum or individual heroics. In operational contexts, wellness infrastructure typically consists of durable roles, predictable reflection cycles, shared baseline literacy, and clearly defined escalation pathways that function independently of leadership attention or personal availability.
In practice, infrastructure-based wellness tends to take forms that remain functional even when wellness is not an active organizational priority. These structures reduce chronic strain that drives crisis demand. They operate quietly, often invisibly, stabilizing systems without interrupting operations. Importantly, infrastructure complements intervention rather than competing with it.
Stewardship as the Bridge Between Time Horizons
Durable systems rely on identifiable stewards. A steward is not a replacement for leadership authority or clinical expertise. Instead, stewardship maintains continuity across years in environments dominated by short-term demands. In practice, stewardship may be embedded within an existing role, assigned to a single individual with protected continuity, or distributed across a small group with shared responsibility — provided the function remains identifiable and durable. Stewards hold institutional memory, preserve intent through leadership transitions, and ensure that long-horizon considerations remain visible even when operational tempo accelerates.
Clinicians, Peers, and Chaplains as Long-Horizon Carriers of Wellness
Clinicians, peer support personnel, and chaplains naturally operate across extended time frames. Their work spans careers rather than shifts, allowing them to observe cumulative patterns that are invisible at the operational level. Chaplains occupy a distinctive position within this group — trusted, present, and often the first point of contact for personnel who would not self-refer to clinical or formal peer support resources. Together, these roles often sustain wellness efforts during periods when leadership attention fluctuates or resources tighten.
Infrastructure Must Support Those Who Carry the Load
Effective support is manifest as an ongoing, elegant collaboration — with peers, clinicians, and chaplains as partners. But there must be an infrastructure to serve as a foundation. Without structure, clinicians, peers, and chaplains are forced to rely on informal coordination and personal resilience. This dependence on availability and goodwill increases burnout and fragmentation. Supporting long-horizon carriers involves reducing coordination burden, clarifying boundaries of responsibility, ensuring predictable activation thresholds, and providing minimal but reliable structural support. These elements prevent informal systems from collapsing into dependence on personal heroics.
Importantly, infrastructure also acknowledges that baseline capacity does not reside exclusively with peers, clinicians, or chaplains. When systems lack mechanisms that support individualized baseline regulation within daily operations, excess strain is routed upward, accelerating overextension of formal support roles.
Measurement as a Translation Layer Between Temporal Horizons
Wellness, resilience, and crisis intervention programs have historically lacked effective measurement components. Measurement serves as a translation mechanism rather than a pure outcome measure or compliance tool. Measurement-based reflection interrupts continuous operations just enough to reorient attention toward long-horizon impact without triggering operational resistance.
In durable systems, measurement mechanisms tend to be infrequent, low-friction, and longitudinal in orientation. Annual or periodic (e.g., quarterly) reflection cycles are sufficient to preserve institutional memory without disrupting daily operations. When designed appropriately, measurement supports alignment rather than evaluation. Its purpose is visibility, not compliance.
Limitations and Future Directions
Integrated continua of care have been recommended over single, one-off interventions (Ruzek et al., 2004; Schoenbaum et al., 2009). Layered wellness models should outperform single mechanisms. Crisis intervention remains essential within a broader continuum. Infrastructure enables longevity without slowing operations. Systems designed for reality are more likely to endure.
The framework presented here is informed by extensive field engagement across diverse operational contexts. Over multiple years, the authors have engaged in sustained organizational-level conversations with hundreds of agencies and thousands of peer support personnel, chaplains, and clinicians working in high-demand environments. These engagements provided repeated exposure to the constraints, failure points, and adaptation patterns that shape wellness efforts in practice. However, these observations were not collected as part of a formal, systematic research protocol and should be understood as formative rather than evaluative.
This paper is intentionally conceptual in scope. Its purpose is to articulate a structural explanation for recurring wellness failures in high-demand organizations and to outline infrastructure-based design principles that can function under persistent operational constraint. As such, it does not prescribe specific programs, training models, or implementation sequences.
Several limitations follow from this approach. First, the paper does not present empirical evaluation of specific infrastructure configurations. Their relative effectiveness across organizational types, sizes, and operational contexts warrants systematic study. Second, this framework does not address the full range of individual-level interventions or clinical practices relevant to wellness. Crisis intervention, peer support, chaplaincy, and clinical care are treated as essential and enduring components, but their internal structures and comparative efficacy fall outside the scope of this paper. Third, the paper focuses primarily on organizational survivability rather than individual outcome metrics.
Future work may extend this framework through applied studies examining how infrastructure-based wellness operates under varying constraints. Longitudinal research may explore how stewardship, measurement cycles, and baseline capacity preservation influence organizational stability and individual longevity across careers.
By clarifying what this paper does and does not attempt to do, these limitations underscore its central contribution: establishing a design logic that allows wellness systems to endure in environments where attention, time, and resources are perpetually constrained.
References
- Bloomberg Healthcare Efficiency Index. (2020, September). Bloomberg.
- Brown, N. J. (2014). A critical examination of the US Army’s Comprehensive Soldier Fitness program. The Winnower, 2, e143751.
- Brown, N. J. (2023). A critical examination of the US Army’s Comprehensive Soldier Fitness program. Authorea Preprints.
- Commonwealth Fund. (2014, June 16). Mirror, mirror on the wall: How the performance of the U.S. health care system compares internationally.
- Everly, G. S., Jr. (2025). Essentials of psychological crisis intervention, peer support, and the Critical Incident Stress Management system (CISM). ICISF.
- Everly, G. S., Jr., & Mitchell, J. T. (1999). Critical incident stress management (CISM). Chevron.
- Everly, G. S., Jr., & Rosenfeld, R. (1985). Occupational health promotion. Wiley.
- Fikretoglu, D., Liu, A., Nazarov, A., & Blackler, K. (2019). A group randomized control trial to test the efficacy of the Road to Mental Readiness (R2MR) program among Canadian military recruits. BMC Psychiatry, 19(326). https://doi.org/10.1186/s12888-019-2287-0
- Green, L. W., & Kreuter, M. W. (1980). Health promotion planning: An educational and environmental approach. Mayfield Publishing.
- Leppin, A. L., Bora, P. R., Tilburt, J. C., Gionfriddo, M. R., Zeballos-Palacios, C., et al. (2014). The efficacy of resiliency training programs: A systematic review and meta-analysis of randomized trials. PLoS ONE, 9(10), e111420.
- Mitchell, J. T., & Bray, G. (1989). Emergency services stress. Brady.
- Peterson-Kaiser Health Tracker. (2022). Peterson Center on Healthcare & KFF.
- Ruzek, J. I., Young, B. H., Cordova, M. J., & Flynn, B. W. (2004). Integration of disaster mental health services with emergency medicine. Prehospital and Disaster Medicine, 19(1), 46–53.
- Schoenbaum, M., Butler, B., Kataoka, S., Norquist, G., Springgate, B., Sullivan, G., Duan, N., Kessler, R. C., & Wells, K. (2009). Promoting mental health recovery after Hurricanes Katrina and Rita: What can be done at what cost? Archives of General Psychiatry, 66(8), 906–914.